The Medical Form Template – Australia is offered in multiple formats, including PDF, Word, and Google Docs. These files are both customizable and ready for printing, ensuring they fulfill your requirements effortlessly.
Medical Form Template – Australia Editable | PrintableSample
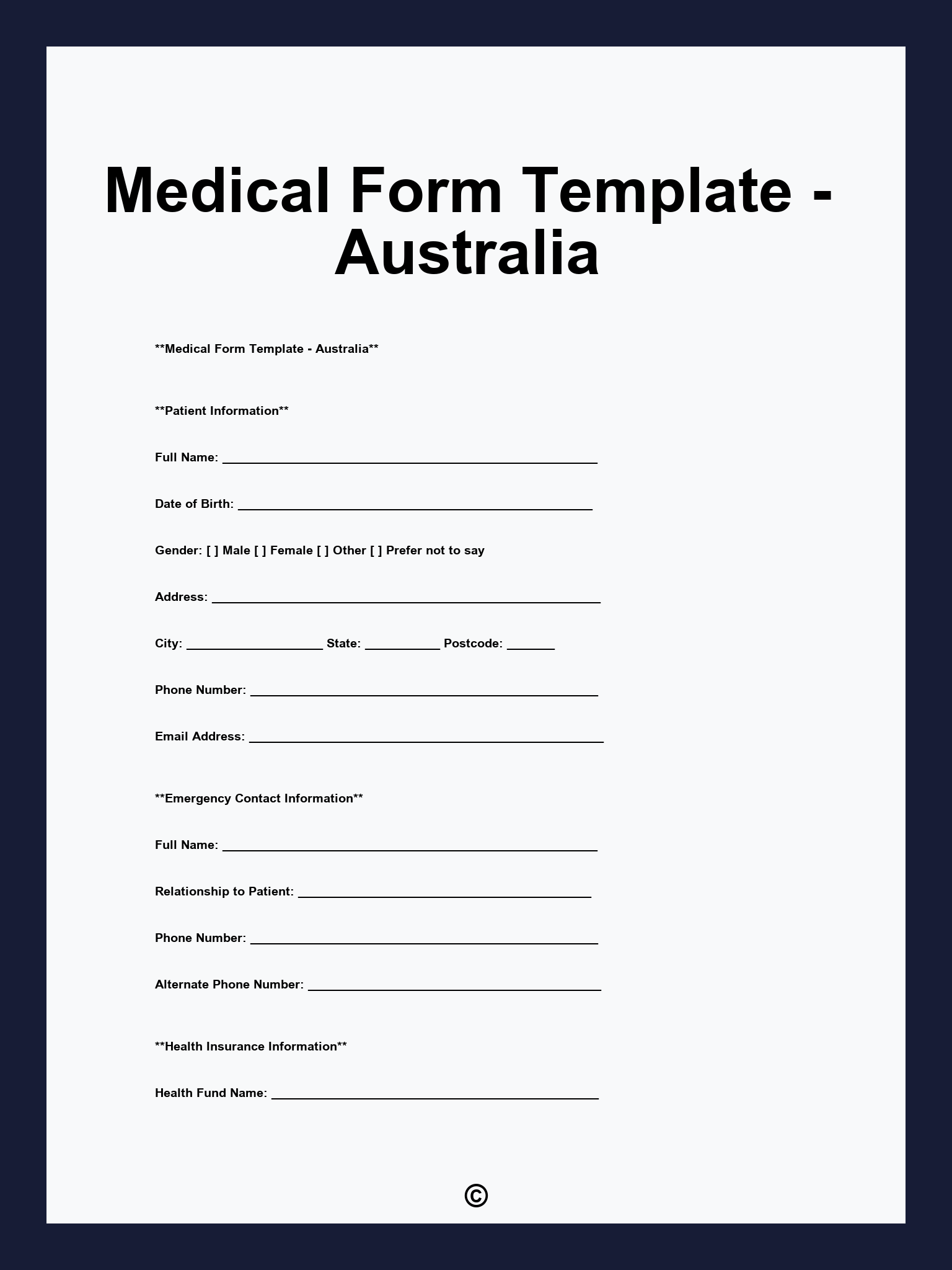
1. Patient Information 2. Emergency Contact Information 3. Medical History 4. Current Medications 5. Primary Care Physician 6. Reason for Visit 7. Consent for Treatment 8. Acknowledgment of Policies 9. Signatures and Acceptance
PDF
WORD
Examples
[Patient’s Name]
[Patient’s ID]
[Patient’s Address]
[Patient’s Phone]
[Patient’s Email]
[Contact’s Name]
[Contact’s Relationship]
[Contact’s Phone]
Please list any previous medical conditions, surgeries, or ongoing treatments: [Details]
Please list any known allergies including medications, food, or environmental: [Details]
Please list any medications you are currently taking, including dosage and frequency: [Details]
[Description of Symptoms or Purpose of Visit]
I, [Patient’s Name], consent to the collection and use of my personal health information for the purpose of providing medical care. I acknowledge that I have received information about my rights regarding my health information.
[Patient’s Name]
[Patient’s Name]
[Patient’s ID]
[Patient’s Address]
[Patient’s Phone]
[Patient’s Email]
[Physician’s Name]
[Physician’s Phone]
[Physician’s Specialty]
[Contact’s Name]
[Contact’s Relationship]
[Contact’s Phone]
Please provide details of any chronic illnesses, surgeries, or significant medical events: [Details]
List any allergies or adverse reactions to medications or treatments: [Details]
Please describe your current health status and any symptoms you are experiencing: [Details]
List any current medications, including over-the-counter and supplements: [Details]
[Description of Symptoms or Reason for Consultation]
I, [Patient’s Name], certify that the information provided is accurate and complete to the best of my knowledge. I consent to the use of my information for medical purposes.
[Patient’s Name]
Printable